When people start looking into growth hormone peptides, they usually focus on which peptide to take, how strong it is, or how fast results will show up. But one of the most important factors is often much simpler: timing. Growth hormone is not released evenly throughout the day. Instead, it follows a pulsatile rhythm, and in adults, one of the most reproducible growth hormone pulses occurs shortly after sleep begins, during the first phase of slow-wave sleep.
That is why growth hormone support is not only a conversation about the compound itself. It is also a conversation about when you take it, what your sleep looks like, and whether your daily habits are helping or interfering with the signal you are trying to support.
What Growth Hormone Peptides Are Really Supporting
A helpful way to think about growth hormone peptides is that many of them are not trying to replace your body’s rhythm. They are trying to work with it. Growth hormone secretion is naturally pulsatile, and sleep onset is one of the strongest anchors of that rhythm. In adults, the most reproducible pulse happens shortly after falling asleep, especially during early slow-wave sleep. [1]
That matters because repair, recovery, and metabolic regulation are all tied to overnight physiology. So when someone uses a peptide at night, the goal is often not to force a brand-new process. The goal is to support a signal that is already built into the body’s normal rhythm. [1]
Why Nighttime Often Works Best
Nighttime is often emphasized because the body is already shifting into a state of recovery during the first few hours of sleep. That is when growth hormone signaling is most naturally aligned with sleep architecture, especially slow-wave sleep. [1]
Nighttime protocols are often described as working with your body, not against it. If sleep is inconsistent, too short, or poor in quality, the signal itself may be weaker. As a result, someone can follow a protocol consistently and still feel disappointed.
This conclusion is based on the close link between sleep structure and growth hormone release. [1]
Food and Insulin Can Change the Environment
Another major point is the relationship between food, insulin, and growth hormone signaling. The growth hormone and IGF-1 system does not operate in isolation. Insulin is an important co-player in regulating the GH/IGF-1 axis by affecting hepatic growth hormone sensitivity and IGF-1 generation. [2]
That is why food timing becomes such a practical part of the conversation. It is not that eating is bad. It is that late-night eating can change the hormonal environment around a nighttime growth hormone protocol. This is a practical inference from the GH/IGF-1 and insulin relationship rather than a universal rule for every protocol. [2]
This is also why one of the most common mistakes is not necessarily the peptide itself. Often, it is eating too close to dosing, poor sleep, or inconsistent timing. [1][2]
If you want to better understand how metabolic support fits into the bigger picture, you can also read more about how metabolic health support differs from growth hormone support.
The Most Common Mistake Is Not Always the Peptide
One of the strongest takeaways is this: more is not always the answer. A lot of people assume that if they are not seeing results, they need a stronger protocol, a higher dose, or a different peptide. But in many cases, the bigger issue is the environment around the protocol.
If sleep is poor, meals are too close to dosing, alcohol is disrupting sleep architecture, or timing changes from day to day, then the body may never be getting a clean opportunity to respond well. That conclusion follows from the evidence on sleep-related growth hormone release, the GH/IGF-1 axis, and alcohol-related sleep disruption. [1][2][3]
That is what makes this topic so important. The question is often not just: Is this peptide working? The better question is: Is my body being given the right conditions to respond?
What the Comparison Chart Shows
The chart adds an important layer to the conversation because it shows that not all growth hormone peptides work the same way. Some are better understood as secretagogues, some as GHRH analogs, and some as downstream growth-factor signaling agents.
Secretagogues and ghrelin mimetics
This group includes compounds like GHRP-2/6 and ipamorelin. These are used to trigger growth hormone release through growth hormone secretagogue pathways. Ipamorelin has been described in the literature as a selective growth hormone secretagogue with less stimulation of ACTH, cortisol, and prolactin than older GHRP compounds. [4] That supports the chart’s overall framing of ipamorelin as a cleaner, more selective option than older GHRP-style approaches. [4]
GHRH analogs
This group includes sermorelin, CJC-1295, and tesamorelin. These work further upstream in the growth hormone axis by signaling through growth hormone-releasing hormone pathways. Tesamorelin is an FDA-approved growth hormone-releasing factor analog indicated for the reduction of excess abdominal fat in adults with HIV and lipodystrophy. [5] That makes it distinct from general educational discussions of peptides used outside an FDA-approved indication. [5]
The chart’s framing is useful because it shows these peptides as being more about guiding or amplifying the body’s own signaling rather than bypassing it outright. That is especially relevant when comparing shorter-acting options with longer-acting ones. For example, CJC-1295 formulations differ substantially depending on whether they include DAC, which changes how long the compound stays active. [6]
Downstream growth-factor signaling
This is where IGF-1 LR3 is usually placed in the chart. IGF-1 is a major target of growth hormone, but it also has metabolic and tissue-level actions that are distinct from growth hormone itself. [7] That is why the chart treats IGF-1 LR3 differently from the nighttime sleep-linked secretagogues. It fits better as a downstream, targeted signaling category rather than a simple “support your natural nighttime pulse” option. [7]
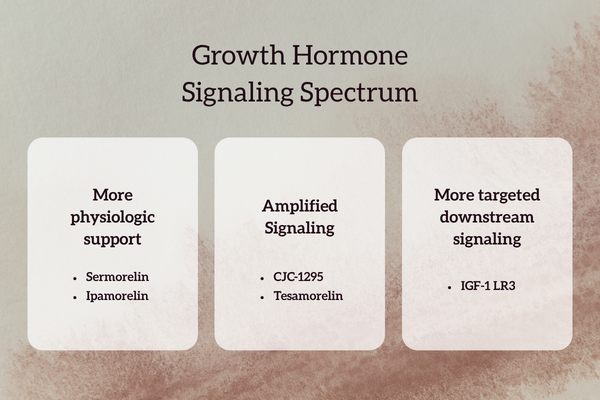
Understanding the Signaling Spectrum
The signaling spectrum graphic helps simplify the chart visually. At the mildest end, it places sermorelin as the most physiologic style of stimulation. That fits with the general idea of a short-acting GHRH analog supporting pulsatile release rather than creating a long sustained elevation.
The graphic then places tesamorelin and CJC-1295 in a more amplified category, reflecting stronger or more prolonged growth hormone signaling. With CJC-1295, the presence or absence of DAC matters a great deal because DAC significantly changes the peptide’s half-life and overall pharmacokinetic profile. [6]
On the more targeted end, the graphic places IGF-1 LR3, which is consistent with the fact that IGF-1 acts downstream of growth hormone and has effects that are not identical to GH itself. [7]
One more useful point from the spectrum graphic is the note that ipamorelin is often paired with CJC or tesamorelin to help extend and strengthen the pulse they initiate. Mechanistically, that pairing makes sense because ipamorelin works through the growth hormone secretagogue pathway, while CJC and tesamorelin work through GHRH-related signaling. [4][5][6]
What Actually Enhances Results
The lifestyle piece still matters, even with the chart. The chart does not replace the basics. It reinforces them.
Sleep quality
Growth hormone release is strongly linked to early slow-wave sleep, so deep, consistent sleep still matters. [1]
Protein intake
Growth hormone may be part of the signal, but the body still needs enough nutritional support to repair and rebuild. That is a basic physiology point and helps explain why signaling alone is not the whole story.
Consistency
If timing changes constantly, it becomes harder to work with the body’s rhythm or evaluate what is actually helping. This is a practical conclusion based on the timing-dependent nature of sleep-linked GH release. [1]
Limiting alcohol
Alcohol can disrupt sleep architecture and alter nighttime sleep patterns. A recent systematic review and meta-analysis found that alcohol changes the characteristics of night-time sleep, including REM-related measures and sleep continuity. [3] Even if someone falls asleep faster, the overall sleep pattern can still become less restorative. [3]
For readers who want to focus on recovery more directly, we also break that down in our guide to supporting recovery before chasing stronger results.
The Real Takeaway
The biggest takeaway is this: this is not always about taking more. It is about taking the right category, at the right time, in the right environment.
Some peptides are milder and more physiologic. Some are stronger or longer acting. Some sit further downstream and do not belong in the same conversation as nighttime secretagogues. But no matter where they sit on the chart, the body still responds best when sleep, timing, routine, and recovery habits are in place. [1][2][3][7]
So the real message is not “take more.” It is to learn what category you are using, what it is actually signaling, and whether your habits are allowing that signal to work. [1][2][7]
The Revive Approach
At Revive With Me, we believe better results come from understanding how the body already works and then supporting that process with more intention. Growth hormone peptides are not just about choosing the strongest option. They are about looking at the full picture, including timing, sleep, recovery, and the type of support your body actually needs.
That is why our approach is centered on education, personalization, and helping you make sense of what each peptide category is really doing. Whether the goal is recovery, body composition, metabolic support, or better overall performance, the conversation should always start with the foundation first.
If you are exploring growth hormone peptides and want a more guided approach, Revive is here to help you understand your options, support your routine, and build a protocol that works with your body, not against it.
References
[1] Van Cauter E, Plat L. Physiology of growth hormone secretion during sleep. Journal of Pediatrics. Review describing how the most reproducible GH pulse in adults occurs shortly after sleep onset and is associated with slow-wave sleep.
[2] Review of the GH/IGF-1 axis describing insulin as an important regulator of hepatic GH sensitivity and IGF-1 generation.
[3] Systematic review and meta-analysis on alcohol and subsequent sleep in healthy adults, describing alcohol-related changes in sleep characteristics and architecture.
[4] Raun K, et al. Ipamorelin, the first selective growth hormone secretagogue. Describes ipamorelin as a selective GH secretagogue with less stimulation of ACTH, cortisol, and prolactin than older compounds.
[5] EGRIFTA prescribing information. Tesamorelin is a growth hormone-releasing factor analog indicated for reduction of excess abdominal fat in adults with HIV and lipodystrophy.
[6] Information comparing CJC-1295 formulations notes important pharmacokinetic differences between DAC and no-DAC versions. This supports the blog’s distinction between longer-acting and more pulse-like versions, though this point is less robustly supported than the primary-source references above.
[7] Review on the metabolic effects of growth hormone and insulin-like growth factor 1, describing IGF-1 as a major target of GH with distinct metabolic actions.